Lesion preparationの重要性: Orbital Atherectomy Systemって?
Orbital Atherectomy for Treating De Novo Severely Calcified Coronary Narrowing (1-Year Results from the Pivotal ORBIT II Trial)
Généreux P, Lee AC, Kim CY, Lee M, Shlofmitz R, Moses JW, Stone GW, Chambers JW.
Am J Cardiol. 2015 Jun 15;115(12):1685-90.
Orbital atherectomy systemというものをご存知でしょうか?
少し古い論文になりますが、ご紹介も兼ねて取り上げたいと思います。BVSの植え込みの際、Lesion preparationの重要性が重要であることに少し触れましたが、Plaque modificationのための、現在日本で使用できるデバイスとしては、Rotational atherectomy, cutting balloon, scoring balloonなどがあります。また近くDCA再導入されるという話も聞きます。しかし、いずれのデバイスも良いClinical outcomeは出せておらず、現在のガイドラインでは、その使用はstent deliveryを補助する場合に限られています。
この論文はOrbital atherectomy system (OAS)がアメリカでFDAの承認を得るに至ったトライアルの結果です。(1)
Orbital atherectomy systemがどんなものかは、You tubeの動画が秀逸なので、百聞は一見にしかず、一度ご覧ください。
https://www.youtube.com/watch?v=PVr7Ftzl5Mc
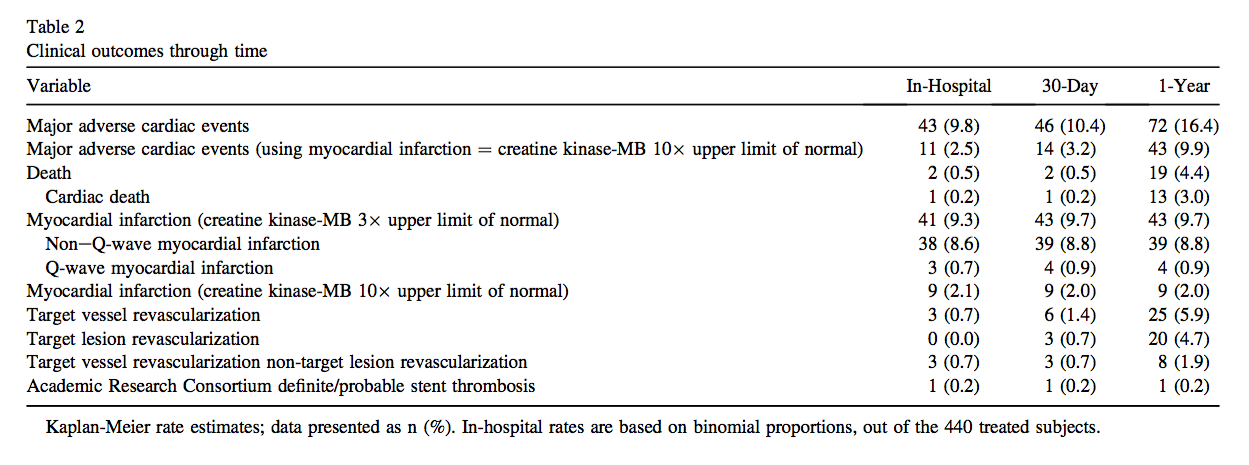
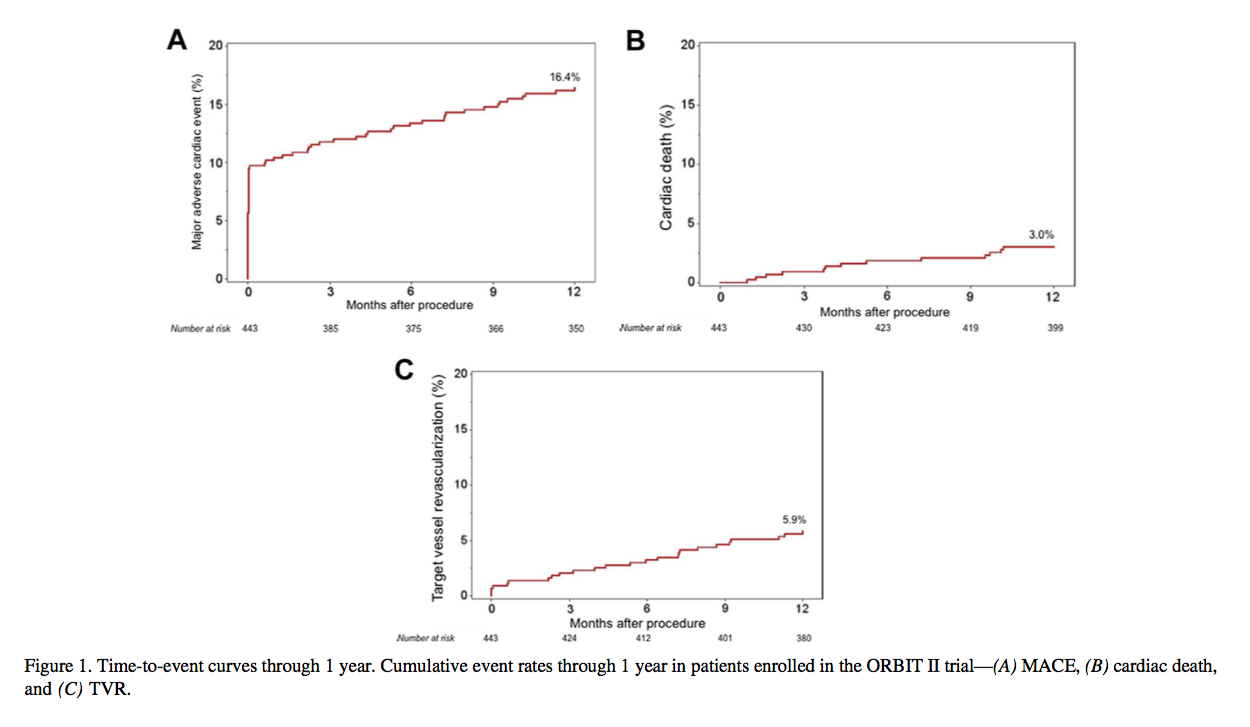
ORBIT II trialはアメリカの49施設で行われたprospective, multicenter, nonblinded clinical trial です。Primary safety endpointは術後30日までのMACE、Primary efficacy endpointはProcedural successでした。この結果はJACC interventionに2014年に発表されていましたが(2)、今回の論文は術後1年での臨床結果です。
OASで治療を行った443人の患者さんを対象にフォローアップ期間16.7か月(中央値)で評価したところ、複合エンドポイント(MACE)は16.4%, 心臓死 (3.0%), 心筋梗塞 (9.7%), TVR (target vessel revascularization) (5.9%)でした。またTLR (target lesion revascularization) は4.7%, ステント血栓症は1名の患者さん(0.2%)で認められました。
この試験自体は対照群がないため、ヒストリカルなデータと比較するしかありませんが、ROTAXUSの9か月のデータと比較しても(TVR 16.7%, TLR, 11.7%, MACE 24.3 %)、ORBIT IIのデータが非常に良かったがことがわかります。(3)
OASにはBurr size 1.25 mmの1種類しかなく、回転速度で切削半径を調節します。(4)そのため、切削半径を調整したい場合にデバイス自体を交換する手間がなく、手技自体の煩雑さが軽減されます。またクラウンの形状を見てもらえればわかりますが、前後のどちらの方向にも切削可能であり、スタックの危険性も低くなります。
ただし、これらの手技自体のメリットでは良好な臨床結果は説明できません。切削の際血管をOcclusionしないことでThermal injuryが生じないことが、ステント植え込み後のNeointimal hyperplasiaの抑制につながり、切削片 (2 μm) がRotablator (5-10 μm)よりも小さいことが心筋障害の低減につながるなど、いくつかそのメカニズムが考えられています。我々も、現在OCTを用いて、そのメカニズムを詳細に検討しているところです。(5-7)
References
1.Genereux P, Lee AC, Kim CY et al. Orbital Atherectomy for Treating De Novo Severely Calcified Coronary Narrowing (1-Year Results from the Pivotal ORBIT II Trial). The American journal of cardiology 2015;115:1685-90.
2. Chambers JW, Feldman RL, Himmelstein SI et al. Pivotal trial to evaluate the safety and efficacy of the orbital atherectomy system in treating de novo, severely calcified coronary lesions (ORBIT II). JACC Cardiovascular interventions 2014;7:510-8.
3. Abdel-Wahab M, Richardt G, Joachim Buttner H et al. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: the randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc Interv 2013;6:10-9.
4. Sotomi Y, Shlofmitz RA, Colombo A, Serruys PW, Onuma Y. Patient Selection and Procedural Considerations for Coronary Orbital Atherectomy System. Interventional Cardiology Review 2016;in press.
5. Sotomi Y, Shammas NW, Suwannasom P et al. Impact of the Orbital Atherectomy System on a Peripheral Calcified Lesion: Quantitative Analysis by Intravascular Echogenicity. JACC Cardiovascular interventions 2015;8:e205-6.
6. Sotomi Y, Shlofmitz RA, Nakatani S, Onuma Y, Serruys PW. Impact of the orbital atherectomy system on a coronary calcified lesion: quantitative analysis by light attenuation in optical coherence tomography. EuroIntervention 2015;11:e1.
7. Sotomi Y, Cavalcante R, Shlofmitz RA et al. Quantification by Optical Coherence Tomography Imaging of the Ablation Volume Obtained with the Orbital Atherectomy System in Calcified Coronary Lesions. EuroIntervention 2016;in press.