PAD領域における過去最大のTrial: EUCLID
今回は自分の留学先であるDuke Clinical Research Instituteが中心となって施行されたEUCLID (The Examining Use of Ticagrelor in Peripheral Artery Disease) trialについて取り上げたいと思います。EUCLID trialはAHA2016のLate Breaking TrialでDCRIのDr Patelより発表され、NEJMに同時掲載されています(N Engl J Med. 2016 Nov 13 Epub ahead of print)1。またrevascularizationに焦点を当てたsub-group analysisに関してもCirculationに同時掲載されています(Circulation. 2016 Nov 13 Epub ahead of print)2。先日、DCRIにおいてもDr PatelおよびDr JonesからEUCLID trialの報告会があり大変盛り上がりました(図1)。

図1. DCRIの報告会で発表するDr Patel
EUCLID trialはPeripheral Artery Disease (PAD) 患者に対するTicagrelor vs. Clopidogrelのガチンコ比較のRCTです。まずは簡単に背景から。
PADに関しては、AHA/ACC guidelineが2016年に改定されています。2016 AHA/ACC guideline (2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease)3 では、Symptomatic PADに対する抗血小板薬としてAspirin単剤およびClopidogrel単剤がClass Ⅰとして推奨されています。Aspirin単剤に関しては、PADに対するAspirin vs. Placeboのメタ解析4においてAspirin投与群はPlacebo投与群と比較して12%の心血管イベントの抑制が認められたという結果が根拠になっています。一方でClopidogrel単剤に関しては、動脈硬化疾患を有する患者に対するAspirin単剤 vs. Clopidogrel単剤のRCT(CAPRIE trial)5においてClopidogrel投与群はAspirin投与群と比較して8.7%の心血管イベントの抑制が得られ、その抑制効果がPAD群において顕著であったことが根拠となっています(図2)。

図2. Aspirin vs. Clopidogrel (元文献はLancet. 1996;348:1329-1339. 図はAHA2016から)
TicagrelorはClopidogrelと同様にP2Y12に拮抗する薬剤ですが,体内での代謝を要さない直接的拮抗薬であり,その拮抗作用はClopidogrelより一貫しているとされています。日本でも薬事承認され今後発売予定ですが、こちらのフェローを話をしていると、急性心筋梗塞での使用はかなり普及している印象です。
さて、TicagrelorのPADに対する効果に関してですが、心筋梗塞の既往を有する患者に対するTicagrelor + Aspirin vs. Placebo + AspirionのRCTであるPEGASUS-TIMI54のsub-group解析6によると、TicagrelorはPAD合併の有無に関わらず心血管イベントの抑制に寄与し、さらにその効果はPAD合併患者においてより顕著だったことが示されています(図3)。またACS患者に対するTicagrelor + Aspirin vs. Clopidogrel + AspirinのRCTであるPLATO trialのPADに関するsub-group解析7においても同様の傾向が認められましたが、TicagrelorはClopidogrelと比較して統計学的に有意な心血管イベントの抑制を示すことはできませんでした(図4)。以上の背景から、PAD患者に特化した抗血小板薬の試験が求められるようになり、EUCLID試験が企画されました。
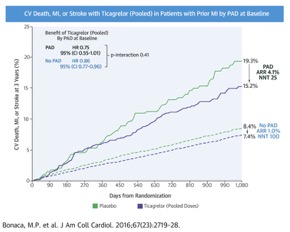
図3. PEGASUS-TIMI54 sub-group analysis (J Am Coll Cardiol. 2016;67:2719-2728.)
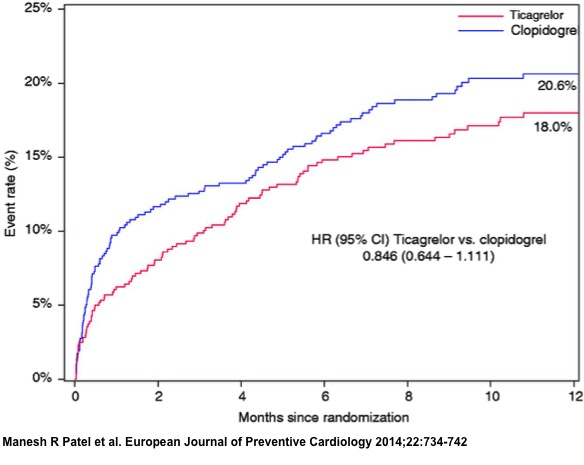
図4. PLATO trial sub-group analysis (Euro J Prev Cardiol. 2015;22:734-742.)
EUCLID trialはSymptomatic PAD患者に対するTicagrelor vs. Clopidogrelのdouble blindおよびdouble dummy試験になります(図5)。
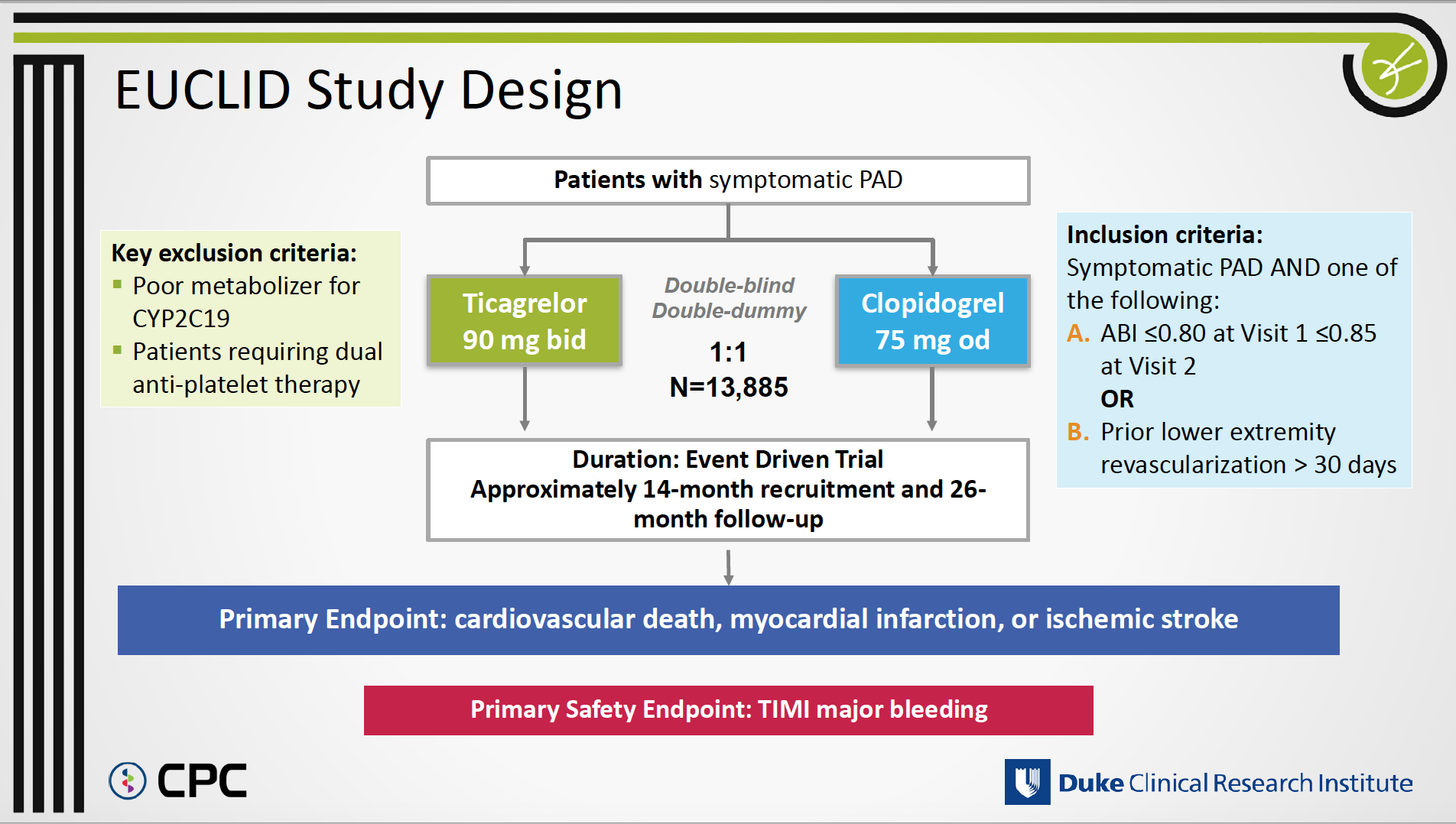
図5. EUCLID trialの概要 (AHA2016より)
試験の主な特徴としては以下の3点が挙げられると思います。
・PAD領域のtrialとして過去最大の症例数であること
・Aspirinを比較対照群として設定しなかったこと
・Clopidogrelのpoor metabolizerであるCYP2C19変異 (two loss of function cytochrome P-450 2C19 alleles)を有する患者群を除外したこと
EUCLID trialは日本を含む28カ国811施設から13,855名がランダム化され、これはPADに特化した試験としては過去最大のものです。これまでのPAD領域における抗血小板薬のエビデンスが動脈硬化疾患全般を対象としたtrialのsub-group解析に依存していた現状を鑑みると、EUCLID trialの意義は限りなく大きいと思われます。
またEUCLID trialにおいてはAspirinを比較対照群として設定せず、Clopidogrelを比較対照群として設定しています。これに関してDCRIの報告会では、「ClopidogrelがAspirinと比較してPAD領域で有効性に勝っていることは周知の事実であり、Clopidogrelに対して優位性を示すことにこそ試験の意義があると判断したため」と言っていました。またPADに対するDAPTの有用性は、動脈硬化疾患を対象としたAspirin単剤 vs. Aspirin + ClopidogrelのRCTであるCHARISMA trial8において、DAPT群はAspirin単剤群と比較して心血管イベントの抑制傾向が認められたものの、有意に出血イベントが多かったという結果が示されており、現時点では否定的です。そのため、EUCLID trialにおいてもTicagrelor + AspirinというDAPTの検証はなされなかったという背景があります。
Primary outcome (CV death + MI + Strole) は図6に示す通り、neutralな結果でした。またALI hospitalizationを含むSecondary outcomeに関しても有意差はなく (厳密に言うとStrokeにおいてのみTicagrelor群にfavorな結果でした)、Safety endpoint (TIMI major bleeding) に関しても同等の結果でした。ただし、投与薬剤の中止に関しては、dyspneaとminor bleedingの影響でTicagrelor群に有意に多いという結果となりました。
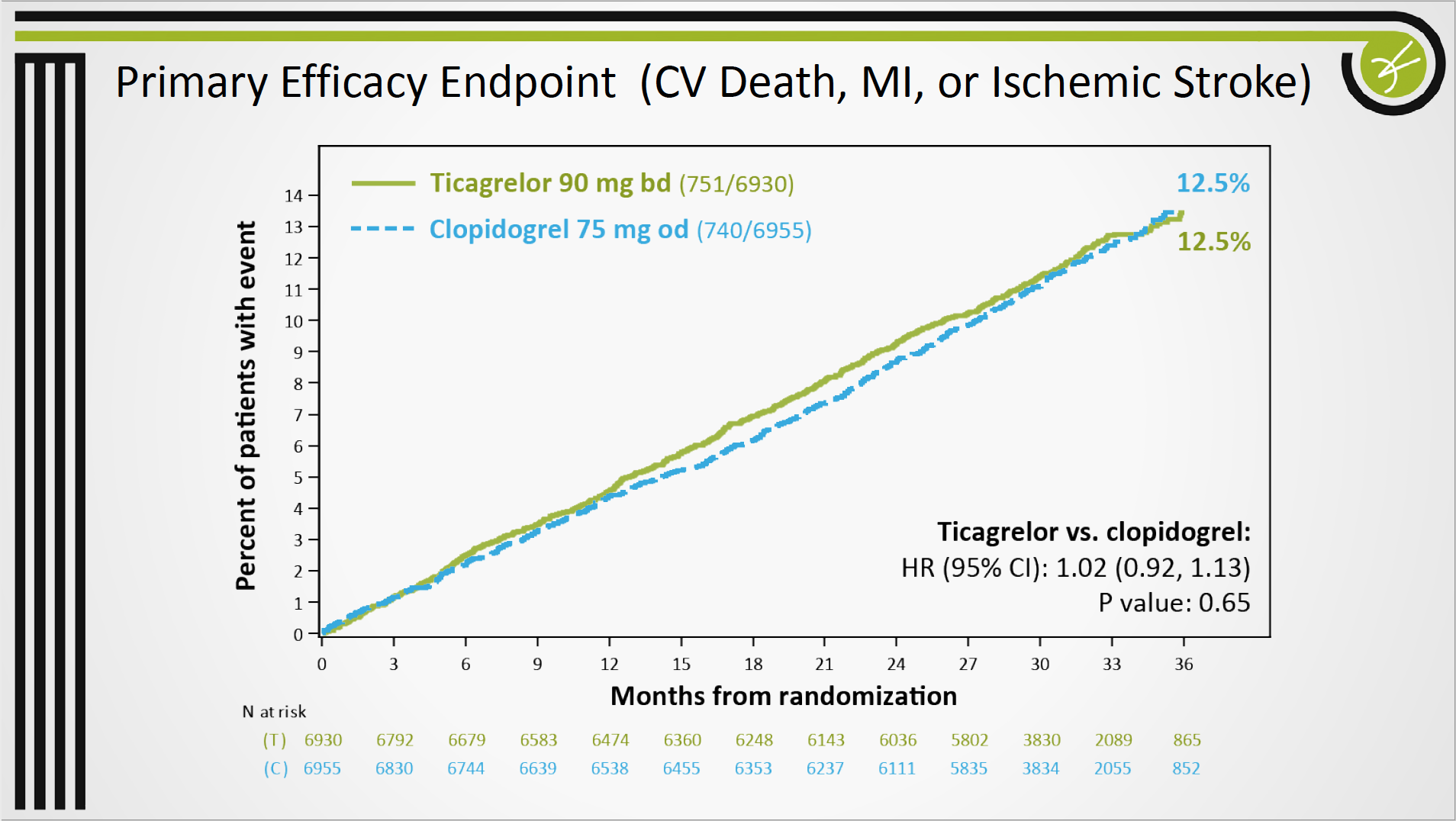
図6. EUCLID trialのPrimary outcome (AHA2016より)
この結果から、PADに対するTicagrelorはClopidogrelと同等と結論づけることになるでしょうか?この点に関しては、やはり個人的にはClopidogrelに対するpoor metabolizerが除外されていることを考慮した方が良いように思います。EUCLID trialでは実に、616名がpoor metabolizer (定義は「two loss of function cytochrome P-450 2C19 alleles」) を理由にランダム化の時点で除外されています。ACS患者に対するTicagrelor + Aspirin vs. Clopidogrel + AspirinのRCTであるPLATO trial では、全患者の27%が「at least one loss of function cytochrome P-450 2C19 allele」であったとされており、その患者群においてClopidogrel群に対するTicagrelor群の優位性が顕著であったと報告されています(図7)9。つまり、EUCLID trialにおいてpoor metabolizerが除外されていなければ、結果は大きく変わっていた可能性が考えられます。特にpoor metabolizerが多いとされる日本においては非常に重要な点と考えらえます。
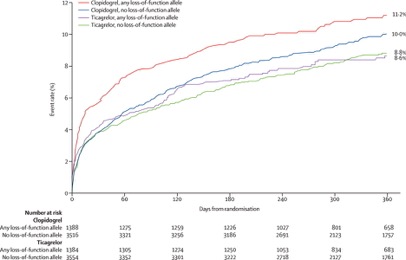
図7. CYP2C19変異の有無に応じたTicagrelor vs. Clopidogrelの成績 (Lancet. 2010;376:1320-1328.)
参考文献;
1. Hiatt WR, Fowkes FGR, Heizer G, et al. Ticagrelor versus Clopidogrel in Symptomatic Peripheral Artery Disease. New England Journal of Medicine. 2016.
2. Jones WS, Baumgartner I, Hiatt WR, et al. Ticagrelor Compared With Clopidogrel in Patients with Prior Lower Extremity Revascularization for Peripheral Artery Disease. Circulation. Nov 13 2016.
3. Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. Nov 13 2016.
4. Berger JS, Krantz MJ, Kittelson JM, Hiatt WR. Aspirin for the prevention of cardiovascular events in patients with peripheral artery disease: a meta-analysis of randomized trials. JAMA. May 13 2009;301(18):1909-1919.
5. Committee CS. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). CAPRIE Steering Committee. Lancet. Nov 16 1996;348(9038):1329-1339.
6. Bonaca MP, Bhatt DL, Storey RF, et al. Ticagrelor for Prevention of Ischemic Events After Myocardial Infarction in Patients With Peripheral Artery Disease. J Am Coll Cardiol. Jun 14 2016;67(23):2719-2728.
7. Patel MR, Becker RC, Wojdyla DM, et al. Cardiovascular events in acute coronary syndrome patients with peripheral arterial disease treated with ticagrelor compared with clopidogrel: Data from the PLATO Trial. European journal of preventive cardiology. Jun 2015;22(6):734-742.
8. Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. Apr 20 2006;354(16):1706-1717.
9. Wallentin L, James S, Storey RF, et al. Effect of CYP2C19 and ABCB1 single nucleotide polymorphisms on outcomes of treatment with ticagrelor versus clopidogrel for acute coronary syndromes: a genetic substudy of the PLATO trial. Lancet. Oct 16 2010;376(9749):1320-1328.