見えすぎちゃうOCT-guided PCIでどこまでやるべき?
Clinical Impact of OCT Findings During PCI: The CLI-OPCI II Study.
Prati F, Romagnoli E, Burzotta F, Limbruno U, Gatto L, La Manna A, Versaci F, Marco V, Di Vito L, Imola F, Paoletti G, Trani C, Tamburino C, Tavazzi L, Mintz GS.
JACC Cardiovasc Imaging. 2015 Nov;8(11):1297-305.(1)
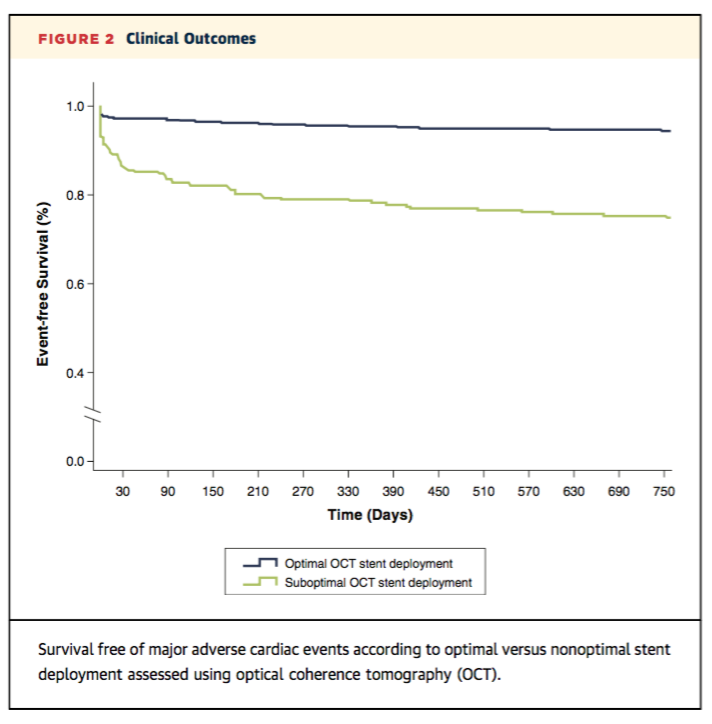
JACC Cardiovasc Imaging からのCLI-OPCI registryの多施設後ろ向き研究のデータです。PCI施行時のOCT 所見とクリニカルアウトカムの関係を見た研究で、832症例1002病変が対象です。31%の病変でSuboptimal stent implantationが認められ、その群ではMACEが有意に多いという結果でした (59.2% vs. 26.9%; p < 0.001)。Suboptimal stent implantation の定義は後述しますが、いくつかの項目があり、そういった所見が1つでもあるとMACEのハザード比は3.53倍になるという結果です (HR: 3.53; 95% confidence interval: 2.2 to 5.8; p < 0.001)。
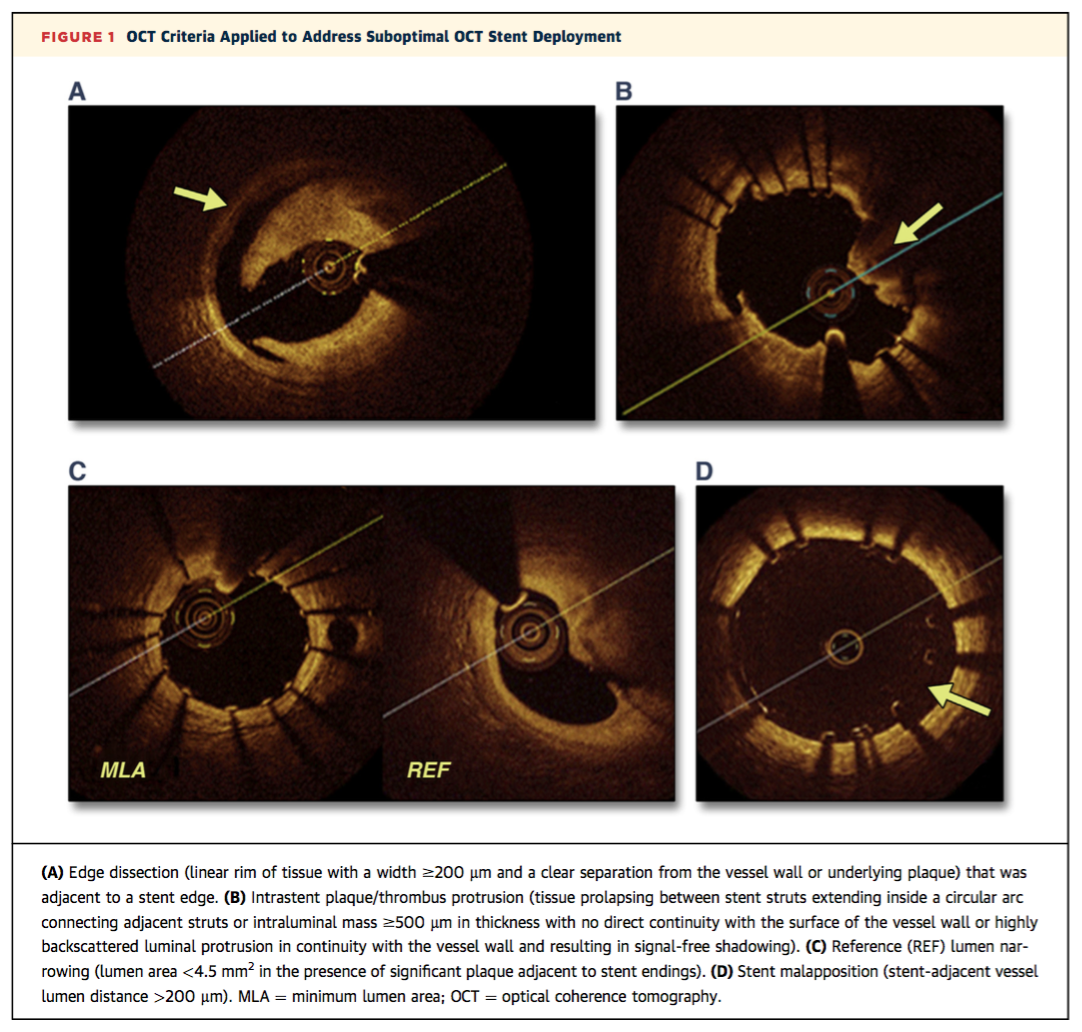
Suboptimal stent implantationは以下のように定義されています。
1. Edge dissection: the presence of a linear rim of tissue with a width ≥200 mm and a clear separation from the vessel wall or underlying plaque that was adjacent (<5 mm) to a stent edge.
2. Reference lumen narrowing: lumen area <4.5 mm2 in the presence of significant residual plaque
adjacent to stent endings;
3. Malapposition: stent-adjacent vessel lumen distance >200 μm
4. In-stent minimum lumen area (MLA) <4.5 mm2;
5. In-stent MLA <70% of the average reference lumen
area;
6. Intrastent plaque/thrombus protrusion: tissue
prolapsing between stent struts extending inside a circular arc connecting adjacent struts or intraluminal mass ≥500 μm in thickness, with no direct continuity with the surface of the vessel wall or highly backscattered luminal protrusion in continuity with the vessel wall and resulting in signal-free shadowing.
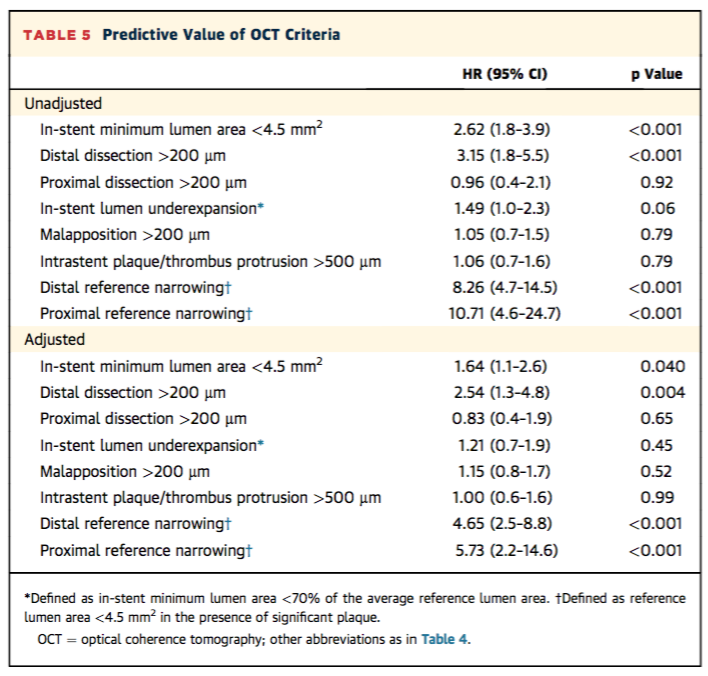
これらの項目の中で、① in-stent minimum lumen area <4.5 mm2 (HR: 1.64; p = 0.040), ② dissection >200 μm at the distal stent edge (HR: 2.54; p = 0.004) ③ reference lumen area <4.5 mm2 at either distal (HR: 4.65; p < 0.001) or proximal (HR: 5.73; p < 0.001) stent edges がMACEの予測因子として統計学的に有意でした。また逆に、in-stent minimum lumen area/mean reference lumen area <70% (HR: 1.21; p 1⁄4 0.45), stent malapposition >200 μm (HR: 1.15; p = 0.52), intrastent plaque/thrombus protrusion >500 μm (HR: 1.00; p = 0.99), and dissection >200 μm at the proximal stent edge (HR: 0.83; p = 0.65) は影響しなかったという結果でした。しかし、これらの項目のうち一つでもあればSuboptimal stent implantationとされ、MACEに関連するという結果でした。
このStudyの結果は、今後のOCTを用いたOptimal stentingにおいて一つの指標となると思いますが、Suboptimal findingsの定義についてはやや議論の余地があるように思います。定義の中に出てくる数字は引用している論文の中にはっきり明記されているものではなく、非常に恣意的に決められた印象があります。
例えば、Malappositionの定義は“stent-adjacent vessel lumen distance >200 μm”とされていますが、通常はステントストラットの厚さによって変わりうるものです。(2) さらに細かい話をすると、Malapposed strutのパーセンテージのカットオフ値なども明記されていません。1病変あたり何百というストラットを通常解析しますが、一個でもそんなストラットがあったらMalappositionにしたかと言うと、そういうわけではないと思います。また、Malapposition distanceが260-270 µm以下であれば慢性期にカバーされるという報告がすでにあり(3,4)、200 μmという数字はやや悲観的かと思います。
In-stent MLA < 4.5 mm2という数字にしても、Stent expansion indexを用いず (5)、一つの数字にしてしまったことは非常にシンプルでわかりやすいですが、そのgeneralizabilityに疑問が生じます。例えばSmall vesselやLeft mainには直接適応できないでしょう。
この定義のことを言い出したらきりがありませんが、アプローチとしては非常に興味深い研究です。個人的には、本研究ではOCT 所見とOutcomeとの関連はMACEでしか評価されていませんが、どのOCT所見がMACEのどの項目と関連していたかが気になるところです。
Optimal stentingの指標としては非常に興味深く、今後のOCT guide PCIの基礎となり得るような報告ですが、本研究の結果を日常臨床にそのまま当てはめるのは少し難しいかもしれません。タイトルにある質問に答えを出すべく、さらなる前向き研究に期待が持たれます。
References
1. Prati F, Romagnoli E, Burzotta F et al. Clinical Impact of OCT Findings During PCI: The CLI-OPCI II Study. JACC Cardiovascular imaging 2015;8:1297-305.
2. Nakatani S, Sotomi Y, Ishibashi Y et al. Comparative analysis method of permanent metallic stents (XIENCE) and bioresorbable poly-L-lactic (PLLA) scaffolds (Absorb) on optical coherence tomography at baseline and follow-up. EuroIntervention 2015;11.
3. Kawamori H, Shite J, Shinke T et al. Natural consequence of post-intervention stent malapposition, thrombus, tissue prolapse, and dissection assessed by optical coherence tomography at mid-term follow-up. European heart journal cardiovascular Imaging 2013;14:865-75.
4. Gutierrez-Chico JL, Wykrzykowska J, Nuesch E et al. Vascular tissue reaction to acute malapposition in human coronary arteries: sequential assessment with optical coherence tomography. Circulation Cardiovascular interventions 2012;5:20-9, s1-8.
5. de Jaegere P, Mudra H, Figulla H et al. Intravascular ultrasound-guided optimized stent deployment. Immediate and 6 months clinical and angiographic results from the Multicenter Ultrasound Stenting in Coronaries Study (MUSIC Study). European heart journal 1998;19:1214-23.