Real worldでは実際のところBVSってどうなの?
1-Year Outcomes of Everolimus-Eluting Bioresorbable Scaffolds Versus Everolimus-Eluting Stents
A Propensity-Matched Comparison of the GHOST-EU and XIENCE V USA Registries
Tamburino C, Capranzano P, Gori T, Latib A, Lesiak M, Nef H, Caramanno G, Naber C, Mehilli J, Di Mario C, Sabaté M, Münzel T, Colombo A, Araszkiewicz A, Wiebe J, Geraci S, Jensen C, Mattesini A, Brugaletta S, Capodanno D.
JACC Cardiovasc Interv. 2015 Dec 30. pii: S1936-8798(15)01757-4. doi: 10.1016/j.jcin.2015.10.042.
Real worldを反映していると何かと引き合いに出されるGHOST-EU registryからのPropensity Score matchingを使ったStudyです。(1) XIENCE V USA Registryの5034症例とGHOST-EUの1189症例からPS matchingさせ、Absorb、XIENCE各群905症例ずつでフォローアップ1年のデータを比較しています。
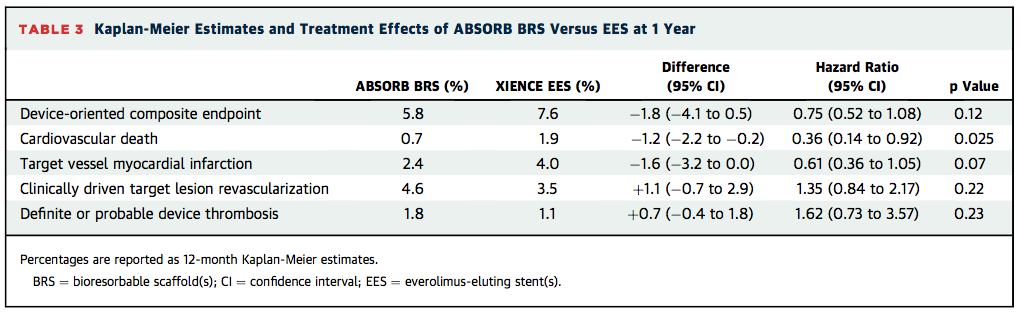
DoCE (device-oriented composite endpoint)はAbsorb 5.8% vs. XIENCE 7.6% (p=0.12)で有意差はなく、Cardiac DeathはAbsorb 0.7% vs. XIENCE 1.9% (p=0.03)となり、Absorb群で有意に低下していました。またAbsorb群ではXIENCE群に比較して心筋梗塞の発症が少ない傾向が認められています。(2.4% vs. 4.0%, p=0.07) 気になるdefinite or probable scaffold thrombosisに差はありませんでした(1.8% vs. 1.1%, p=0.23)。
この結果はLancetに掲載された2本のMeta analysisの結果と相反するものですが、RegistryというReal worldをより反映していると考えられるStudyの結果としては非常に興味深いものです。
ただし、やはりRegistryのPS matching というStudyの特性上、注意するべき点が幾つかあります。
まずPS matchingが適正に行われているかですが、少し気になる点は、マッチングの項目の中にProcedureデータ(後拡張の有無)が含まれていることです。こういったマッチングではアウトカムや治療内容に影響を与えるベースラインのデータのみを使用するのが普通だと思いますし、過去の文献でも次のように述べられています。
“The variables in this list can be selected from reviews of the literature, from prior studies, and from expert opinion. Importantly, the list should only include variables measured at base- line, before exposure. The list should not include the outcome, nor should it include variables in the causal pathway.”(2)
ABSORB II trialで見られた通り、AbsorbとXIENCEでは後拡張のストラテジー(バルーンサイズ、拡張圧)に大きな違いがありましたので(3)、こういったProcedure dataを項目に含むべきかどうかは議論になるところかもしれません。
2点目は、データコレクションについてですが、GHOST-EUでは”site-reported data collection and adjudication”であり、XIENCE V USAでは”centrally adjudicated events and 30% random monitoring”であるということが、アウトカムデータの質の低下、過小評価あるいは過大評価につながる可能性があります。他の70%はどうだったの?ということです。これは仮にPS matchingが適正に行われていたとしても重大なBiasに成り得ます。
論文の中では、その他、Registryの施行時期の違い、DAPTの期間やDrugの種類の違いが与える影響についてもDiscussionされています。Study designによるLimitationが大きいことは否定できませんが、一つ言えることは、少なくともReal worldを反映した非常に興味深いデータであり、現在のAbsorbの治療とXIENCEでの治療とを比較した場合に一方が大きく劣っているということは無さそうな印象です。
References
1. Tamburino C, Capranzano P, Gori T et al. 1-Year Outcomes of Everolimus-Eluting Bioresorbable Scaffolds Versus Everolimus-Eluting Stents: A Propensity-Matched Comparison of the GHOST-EU and XIENCE V USA Registries. JACC Cardiovascular interventions 2015.
2. Austin PC. Propensity-score matching in the cardiovascular surgery literature from 2004 to 2006: a systematic review and suggestions for improvement. The Journal of thoracic and cardiovascular surgery 2007;134:1128-35.
3.Serruys PW, Chevalier B, Dudek D et al. A bioresorbable everolimus-eluting scaffold versus a metallic everolimus-eluting stent for ischaemic heart disease caused by de-novo native coronary artery lesions (ABSORB II): an interim 1-year analysis of clinical and procedural secondary outcomes from a randomised controlled trial. Lancet (London, England) 2015;385:43-54.