BVSのScTの原因ってデバイスじゃなくてテクニックの問題って本当?
Bioresorbable Coronary Scaffold Thrombosis
Multicenter Comprehensive Analysis of Clinical Presentation, Mechanisms, and Predictors
Serban Puricel, Florim Cuculi, Melissa Weissner, Axel Schmermund, Peiman Jamshidi, Tobias Nyffenegger, Harald Binder, Holger Eggebrecht, Thomas Münzel, Stephane Cook, Tommaso Gori.
J Am Coll Cardiol 2016;67:921–31.
Scaffold thrombosis (ScT)の予測因子の検討はイベント数が少ないのでなかなか難しいかもしれませんって最近書いた気がしますが、JACCからScTの予測因子を検討した論文が出ました。
ドイツとスイスの4施設から1305症例(1870 BVS)を対象にフォローアップ期間485日のデータを検討しています。
ScTは42症例で認められ、植え込み後30日まででは1.8%、12か月のデータは3.0%の発生率でした。この数字は、これまでのStudyと比較してもやや高い値です。(1-3)
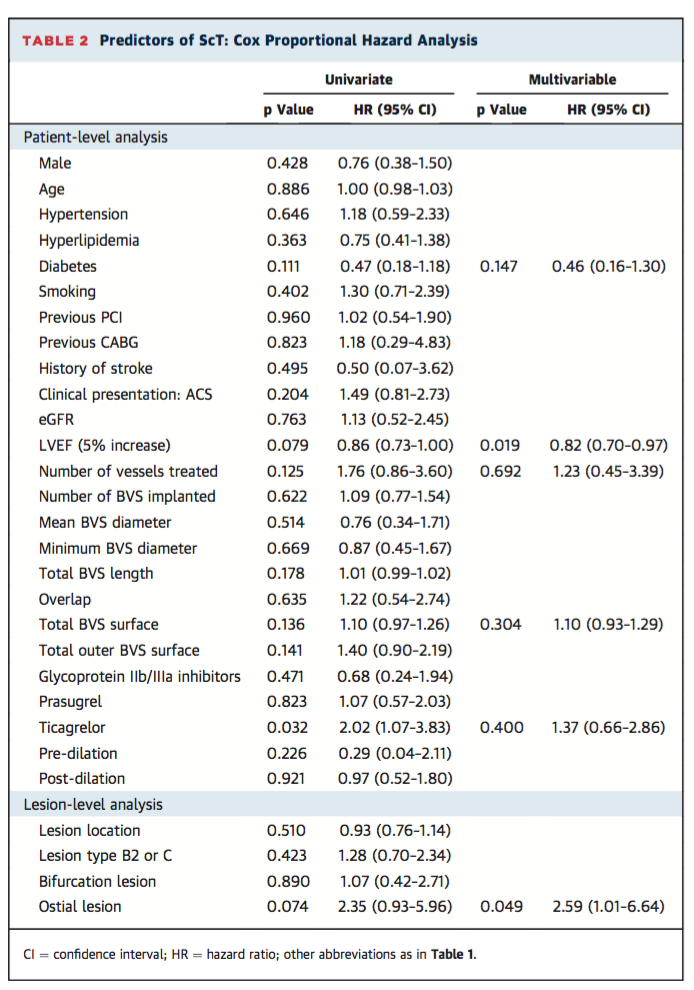
患者背景からの多変量解析の結果、Ostial lesionとImpaired LVEFがScT予測因子となっていますが、そこにProcedureの因子を含めますと、“residual scaled stenosis” (the degree of deployment of the BVS compared with its nominal value)が強く影響してくることがわかりました。
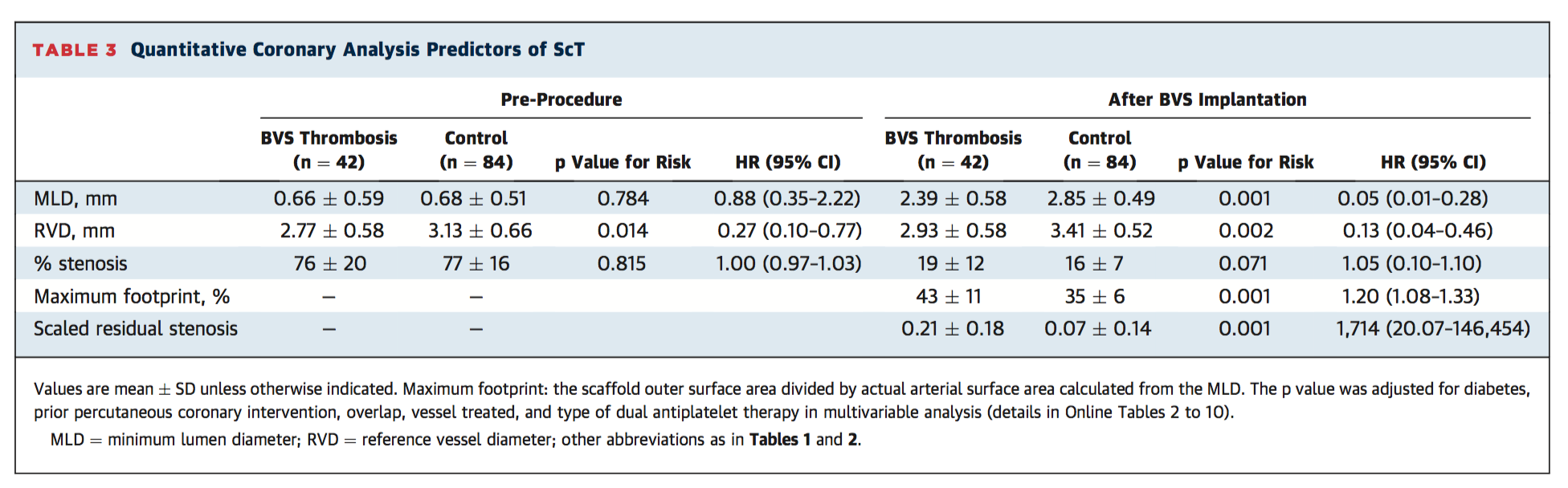
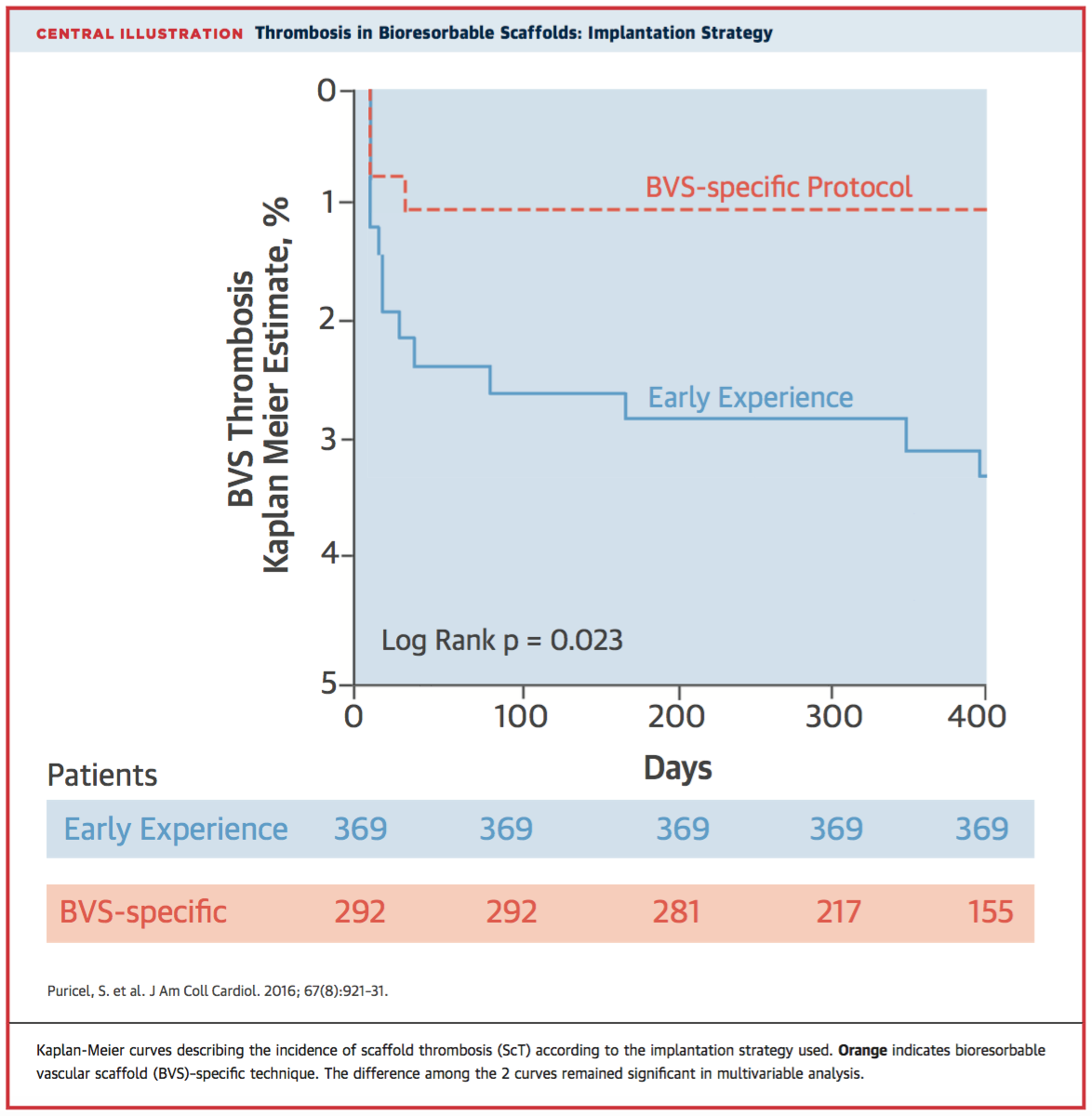
簡単に言うと、Underexpansionがダメっていう理解でいいと思いますが、そうなると、植え込み方法次第でいかようにもできるってことになりますよね。で、この論文の興味深いところはBVS-specific implantation protocolで植え込みを行った群と、そうでない群を比較しています。
BVS-specific implantation protocolの定義は次のようになります。
1. Pre-dilation with noncompliant balloon up to the same size as the RVD (reference vessel diameter).
2. BVS implantation only in case of full expansion of the noncompliant percutaneous transcatheter coronary angioplasty balloon as demonstrated by angiography in 2 orthogonal planes.
3. Implantation of a BVS of the same size as the RVD
at 10 to 12 atm.
4. Post-dilation with noncompliant balloons up to a
maximum of 0.5 mm larger at 14 to 16 atm.
その結果、はっきりと治療ストラテジーの違いがアウトカムに現れてきました。
UnderexpansionがRiskになりそうだということは、Absorob B, EXTEND, IIの結果で既に示されていましたが、(4-6)このスタディで、それが多変量解析によって示され、かつ、それはデバイス自体の問題ではなくて、植え込み方法に問題がある可能性が高いということが示されました。
Retrospective、またこのスタディの一部はCase control studyというデザインのため、結果の解釈には十分注意する必要があります。また、最初に、ScTの予測因子の検討はイベント数が少ないのでなかなか難しいかもしれないと申し上げたことを少し補足しますと、通常こういったロジスティック回帰分析に含んで良い項目の数は、イベント数 / 10 までとなります。なので、42症例というScTのイベント数を考えますと、4項目が限界のはずなのですが、それをはるかに超える予測因子をモデルに組み込んでいるので、統計学的な信頼性については若干の疑問が残ります。
ですが、近年欧米で強く意識されるようになった、BVS植え込み時のDevice selection, Lesion preparation, Post-dilatationの重要性が、このスタディではっきり示された、ということには疑問はありません。そして、この結果は、実際に患者さんへBVSを使用する際には、必ず頭に入れておく必要があります。
References
1. Capodanno D, Gori T, Nef H et al. Percutaneous coronary intervention with everolimus-eluting bioresorbable vascular scaffolds in routine clinical practice: early and midterm outcomes from the European multicentre GHOST-EU registry. EuroIntervention 2015;10:1144-53.
2. Gori T, Wiebe J, Capodanno D et al. Early and midterm outcomes of bioresorbable vascular scaffolds for ostial coronary lesions: insights from the GHOST-EU registry. EuroIntervention 2015;11.
3. Kraak RP, Hassell ME, Grundeken MJ et al. Initial experience and clinical evaluation of the Absorb bioresorbable vascular scaffold (BVS) in real-world practice: the AMC Single Centre Real World PCI Registry. EuroIntervention 2015;10:1160-8.
4. Ishibashi Y, Nakatani S, Sotomi Y et al. Relation Between Bioresorbable Scaffold Sizing Using QCA-Dmax and Clinical Outcomes at 1 Year in 1,232 Patients From 3 Study Cohorts (ABSORB Cohort B, ABSORB EXTEND, and ABSORB II). JACC Cardiovascular interventions 2015;8:1715-26.
5. Serruys PW, Chevalier B, Dudek D et al. A bioresorbable everolimus-eluting scaffold versus a metallic everolimus-eluting stent for ischaemic heart disease caused by de-novo native coronary artery lesions (ABSORB II): an interim 1-year analysis of clinical and procedural secondary outcomes from a randomised controlled trial. Lancet 2015;385:43-54.
6. Abizaid A, Ribamar Costa J, Jr., Bartorelli AL et al. The ABSORB EXTEND study: preliminary report of the twelve-month clinical outcomes in the first 512 patients enrolled. EuroIntervention 2015;10:1396-401.